
BeachPeel Melasma
Melasma is a common, acquired and recalcitrant hyperpigmentation disorder affecting with a higher prevalence females and darker skin types. According to Ogbechie-Godec OA et al (2017) the estimated prevalence of melasma in the general population is at 1% but in higher-risk populations at 9–50%. The known etiologies are various such as UV exposure, hormonal influences, genetics, drugs etc.. Clinically, this pigmentation disorder imposes as multiple bizarre configurated patches located centrofacially, as well as on other sun exposed areas such as neck, décolletage and possibly on lower arms and legs. Consecutively melasma shows histologically an increased melanin content either epidermally or dermally or in both levels. So melasma is a consequence of hyperfunctional melanocytes leading to excessive melanin deposition in the epidermis and dermis. Additionally and in some cases, melasma goes along with increased vascularity of dermal blood vessels as well as possibly with the typical signs of skin aging such as solar elastosis; occasionally, perivascular lymphohistiocytic infiltrates may occur.
This skin disease does not only have a huge impact on the aesthetic look of a patient but certainly on the psychological wellbeing and condition of our patients. Unfortunately, it remains a substantial challenge to effectively and safely treat melasma and moreover to find a safe and effective way to manage melasma on the long term as this disease tends to reoccur. As discussed by the abridged Cochrane review published in the J Am Acad Dermatol in 2014, “a meta-analysis was not possible because of the heterogeneity of treatments” and “randomized controlled trials on well-defined participants with long-term outcomes are needed” to find a consensus on how to treat melasma at best.
Those facts given and being a dermatologist suffering from melasma myself, I started my clinical research on treating melasma by topicals in the late 1990s to find a safe and effective treatment method as well as the optimal therapeutic concept to manage and control melasma for the skin prone to melasma on a longterm perspective.
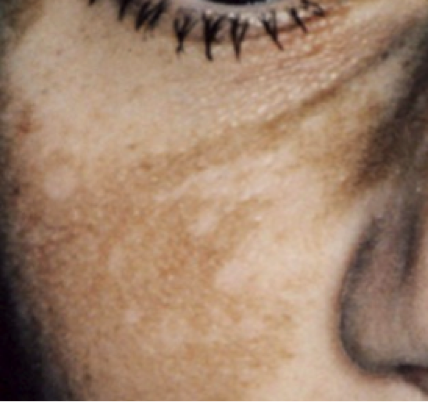
Pic 1. Melasma, ©Dr. Sabine Zenker, Dermatologist
Treatment Principles
The strategy here is, to effectively downregulate melanogenesis by topicals by controlling its formation on various levels (Briganti S et al 2003): Before melanin is formed, the transcriptional control of the tyrosinase expression or the reduction of melanogenic mediators (alpha-MSH) could be in the target. A good example for a topical here is tretinoic acid, the carboxylic acid form of vitamin A, all-trans retinoic acid (ATRA) as it acts on retinoid-activated transcription factors, interferes with melanocyte development and melanogenesis, stimulates the differentiation of melanocyte precursors and removes differentiated melanocytes thanks to its exfoliating capacity. Besides Tretinoin, derivatives such as e.g. retinyl palmitate (the ester of retinol and palmitic acid), retinol (vitamin A1, axerophthol) are frequently used in cosmeceuticals.
During melanin synthesis, blocking of important enzymes involved in melanogenesis such as tyrosinase and peroxidase as well as ROS scavenger inhibition is a common strategy. The gold standard here is undoubtedly hydroquinone HQ: this drug is well known for its suppressive effect on melanin synthesis. As its hydroxyphenolic compound is structurally similar to precursors of melanin the mode of action is predominantly defined by being a competitive inhibitor of tyrosinase. So hydroquinone effects the formation of melanin as well as the degradation of melanosomes, hydroquinones’ efficacy is dose-dependent and so are its side effects such as most commonly mild irritation or contact dermatitis, „confetti“-like hypopigmentations, exogenous ochronosis. So far no malignancy is related to topical HQ use. Arbutin is a naturally occurring HQ b-d-gluconopyranoside, derived from leaves of different berries (bearberry, cranberry etc.). It decreases the tyrosinase activity without affecting messenger RNA (mRNA) expression, inhibits 5,6-dihydroxyindole-2-carboxylic acid (DHICA) polymerase activity (pmel17/silver protein) and exerts inhibitory effect on melanosome maturation. Kojic Acid KA, 5-Hydroxy-2-Hydroxymethyl-4-Pyrone, is a natural substance produced by fungi or bacteria (Acetobacter, Aspergillus, Penicillium). It inhibits the free tyrosinase by chelating copper. ROS scavengers in this context typically are acelaic acid, originally isolated from Pityrosporum ovale is known for its melanin production inhibition, too. Phenylethyl Resorcinol is a potent non-irritant anti-oxidant with the potential to reduce melanin synthesis and to supresses inflammation by inhibiting cox-II-tyrosinase and other inflammatory melanin activating factors. Ascorbic acid interferes with the different steps of melanization, interacts with copper ions at the tyrosinase active site and reduces dopaquinone and by blocking DHICA oxidation. After melanogenesis, melanosome transfer inhibition and melanin dispersion are the two major strategies to reduce unwanted pigmentation and melanin content respectively. Predominantly acids to peel of the skin are mainstays in the topical therapy of melasma: Alpha- and Beta-Hydroxy Acids effect a desquamation of the stratum corneum and dispersion of melanin and they improve the penetration of other agents. Niacinamide has anti-inflammatory properties and is able to decrease the transfer of melanosomes.
Bleach-Peeling Melasma -My Individual Treatment Approach
Knowing about the potential of the described topicals, it immediately suggests that combining them for topically treat melasma makes sense. The strategy is to effect a controlled skin turnover and to combine this with the controlled break down of the unwanted hyperpigmentation. The treatment protocol has to necessarily be flanked by adequate skincare: Cosmeceuticals serve predominantly as protection and hydration; compounded formulations serve as pre- and post-peel-care to prepare the skin for the treatment or to increase the therapeutic effect consecutively.
For the treatment procedure itself, the respective compounds have to be selected individually and based on various factors such as characteristics and severity of the melasma formation, duration of the disease, eventual pre-treatment, recent treatments or treatments from years back, photo-type, skin type, patient`s expectations and considerations in regards to downtime. As a general rule, one has to take into account that e.g. higher concentrations of the working agents or the fact that some actives are regulated as prescription drugs will result in higher efficacy but also longer downtime. But also different regulations such as e.g. restrictions on the use of hydroquinone in countries such as Asia demand alternative compositions for the individual treatment.
A good example for a HQ-free treatment option are ready-to-use compositions such as a specialist combination peels. Typically, such peels combine actives such as kojic acid, alpha-arbutin, azelaic acid, a tyrosinol complex, vitamin C, niacinamide, retinyl palmitate, salicylic acid etc.. such as in Dermamelan©.
Pic 2. Melasma Treatment ©Dermamelan
A medical treatment to bleach-peel the skin can be typically based on the combination of prescription drugs such as hydrochinon, Tretinoin, etc with acids such as Salicylic Acid, Alpha-Hydroxy etc.

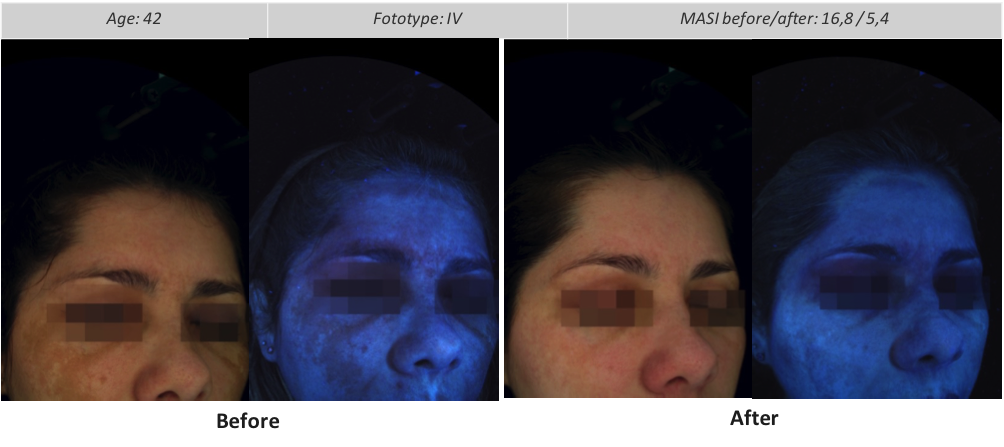
Pic 3. Melasma –Before Bleach-Peel. DrZenkerDFP, Dr. Sabine Zenker, Dermatologist

Pic 4. Melasma –After Bleach-Peel DrZenkerDFP©, ©Dr. Sabine Zenker, Dermatologist
Overall, any patient has to understand that every skin prone to melasma formation needs an individual skin “diet”, meaning that one should be very careful in choosing the respected skincare as many ingredients in cosmetics as well as their treatments as the “wrong” treatment can increase the risk of aggravation or induction of unwanted pigmentation as well as induce post inflammatory. And that skin type-adapted SPF every day throughout the year is utmost essential!
Personal Profile Sabine Zenker, MD, Dermatologist
Sabine Zenker, MD, is a world-renowned Board Certified German Dermatologist who combines her dermatological expertise with a distinct sense for facial and body aesthetics.
Since establishing her private practice DrZenkerDermatology in Munich, Germany, Maximilian Street, in 2003, Sabine Zenker dedicates her daily work to diligent individual patient care as well as to clinical research for established, innovative and pioneering, non- and micro-invasive aesthetic procedures. Since more than 15 years, Dr. Zenker is an in-demand speaker, trainer and consultant by leading medical societies, university and congress organizers around the globe. Contributing to both, the specialist press as well as to consumer magazines, she is widely and regularly quoted in major publications. Zenker is a frequently consulted expert by major media to offer scientific opinions on dermatology and aesthetic dermatology. Sabine Zenker is a certified member of the German, European and the American Society of Dermatology and notable others. By working in her practice and passing on her knowledge, she consistently pursues her goal to help every patient at best.
For more information, please visit www.dr-zenker.de.

Tagged: Clinical dermatology & dermatologic surgery, Peelings, mesotherapy & needling
Rate this article
Share this article on