
Laser treatment of Nevus Ota and Ito
Disorders of hyperpigmentation is one of the most common reason for which patients visit dermatology offices. Hyperpigmentation can be a physiological process, can result from inherited disorders, or pathological process, such as metabolic or neoplastic conditions. At cellular level, pigmentation can result from an excessive production of melanin, increase the numbers of melanosomes and melanocytes; or both. Melanin is produced and stored by melanosomes. These pigmented structures can be found in epidermis, dermis, or both.
Advances in laser technology had led to the discoveries of various laser types and principles to target pigmented lesions, namely melanin. Many of these principles are based on what we call selective photothermolysis. This concept is dated back to the early 1980s, and in vivo result showed the precise selectivity of thermal damage to certain structures inside the skin. Chromophores in the skin, like melanin in pigmented lesions, can specifically absorb certain wavelengths of lasers. This is achieved by a selective light absorption that mainly targets the chromophore, without distributing the heat and damaging surrounding structures.
Melanin has a broad spectrum of laser light absorption, which makes it susceptible to various wavelengths of laser. However, choosing a wavelength that is better absorbed by melanin, and not by other chromophores, such as hemoglobin, is the best choice. Looking at the absorption curves (Figure 1), it is evident that on the melanin absorption curve, shorter wavelengths are highly absorbed by the melanin and longer ones are less absorbed by melanin. This leads to the fact that the longer the wavelength, the deeper the penetration. For example, if the pigmented lesion is mainly epidermal, laser with shorter wavelength might be appropriate, while deeper dermal lesions, is best be treated with a longer wavelength. The same principle does not apply on other chromophores like the water where the absorption curve is ascending which means the shorter the wavelength, the less the absorption is and hence the deeper the penetration is.
Melanosomes has a TRT of about 70-250 nanoseconds, which make Q-switched lasers a good choice to target melanosomes, as it has an ultrashort pulse.
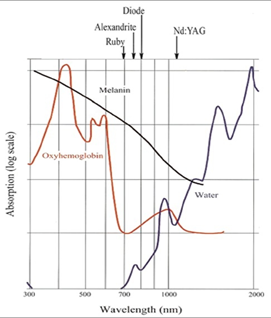
Figure 1. Laser absorption curves showing the different skin chromophores and its absorption coefficient at different wavelengths.
Quality switched, “Q-switched” (QS) laser give pulses in the nanoseconds. This technology produces nanosecond pulses by releasing laser energy in a very short time. Tiny structures like tattoo ink or melanin particles require very short pulse durations in the nanosecond or picosecond (PS) range which lead to very rapid heating of the target that leads to tattoo ink or melanin particles fragmentation. This is caused by acoustic waves which lead to mechanical destruction of the target [7, 8]. Although the exact mechanism of tattoo removal is unknown, it appears that laser treatment leads to alteration in the properties of the pigments, partly by destruction and partly by thermal, photochemical, or photoacoustic means. Histologic and electron microscopic analyses of biopsies indicate disintegration of pigments into smaller fragments which were then phagocytosed by macrophages or carried away via the lymphatic system.
Ruby, Alexandrite, and Nd:YAG lasers can be used in the longer pulse width mode, predominantly for hair removal. Although they have the same wavelengths as the QS lasers used in the treatment of pigmented lesions, they deliver the laser energy over milliseconds rather than nanoseconds. The longer pulse width causes less damage to the melanosomes but they are able to remove some pigmented lesions within the epidermis.
Nevus of Ota, nevus of Ito and nevus of Hori
Nevus of Ota, nevus of Ito and nevus of Hori are special melanocytic nevi that have a slate-brown or blue/grey coloring. They are pigmented disorders characterized by its heterotopic melanocytic dermal location and by blue brown unilateral and sometimes bilateral facial patch in case of nevus of Ota (Figure 2), and in the supraclavicular, scapular, and deltoid region in case of nevus of Ito. It is more common in patients with Asian and black ethnic group. An acquired variant is called Hori’s nevus with more bilateral facial distribution, similar to melasma. Dermal melanocytosis can also occur elsewhere on the body, including inside the mouth.
Despite its benign nature, patients frequently seek an efficient therapy because of its facial involvement.

Figure 2. Nevus of Ota.
QS lasers are used effectively to treat these lesions. The number of treatment sessions correlates with clinical improvement. Post laser hypo and hyperpigmentation are common side effect mainly affecting darker skin patients. In a case series of 19 Korean patients of nevus of Ota with Fitzpatrick skin type IV, 1064 nm Nd:YAG laser was used with low fluence (2.5 J/cm2) with two weeks treatment intervals. The mean number of treatment sessions was 17.1 (range 6 - 32). Among the 19 patients, 18 reached near total clearance. Five patients complained of delayed eyelid response. Post-therapy hyperpigmentation was observed in one patient. In another study, the QS ruby 694 nm laser with 5-7 J/cm2 fluence, 4.0 mm spot size, and 30 ns pulse duration was assessed retrospectively for the treatment of nevus of Ota. The majority of patients had ≥75% clearance with a mean number of 3.5 treatment sessions for children and 5.9 sessions for adults.
Laser and Light Treatment
The efficacy of alexandrite QS laser to treat Ota nevus was reported in 1992, soon followed by numerous publications reporting efficacy of other QS lasers, i.e. Nd:Yag and ruby laser.
Today, the 1064 nm Nd:Yag laser appears as the most efficient comparing the balance between efficacy and side-effects. Due to the deflection to near infra-red of the 1064 nm band emission in the melanin light absorption spectrum, the less absorption by the epidermal melanin layer minimizes the risk of hypochromia, especially in three-five skin type phototype patients. Moreover, the 1064 nm wavelength is the more penetrating among the whole range of QS lasers. Due to the high levelled energy ranges used, and the facial location of the lesions, treatment of Ota nevus by QS lasers is painful and topical anesthesia is required. According to the high leveled fluences used for the treatment of Ota nevus, we recommend treating with the smaller disposable pulse diameter to limit the dermoepidermal split subsequent to the treatment and hence limit any risk of scarring. Pulses are placed in an adjacent, non-overlapping pattern. Immediate skin whitening after the irradiation is followed by oedema and pinpoint bleedings in the minutes following the treatment. Crusts occur in the day following the irradiation and last for up to 10 days. We recommend a minimum of 2 months between sessions on the same area to limit the risk of scarring. The development of a new generation of QS lasers, the picosecond lasers, seems to have not significantly modified the prognosis of the treatment of Ota nevus except perhaps by being followed by a shorter downtime and by decreasing the incidence of hypopigmentation.
Practical Pearls
Skin type is an important factor to consider when treating pigmented lesions as patients with darker skin are more likely to develop hyperpigmentation or hypopigmentation after laser treatment. Therefore, 1064 nm Nd:YAG laser treatment should be considered when treating darker skin type.
The two factors that affect the depth of penetration of laser light are the wavelength and spot size. Longer wavelengths penetrate deeper into the skin and are less scattered. Small spot size will result in a greater proportion of the light being scattered as the light scatters at the edge of the field and will not reach significant depths in the skin. Therefore, increasing spot size could be used instead of increasing the fluence as higher fluences could cause more damage and scarring.
A test spot with the laser provides an opportunity to test the suitability of a particular laser for a skin phototype. The small test area can then be reevaluated in 6-8 weeks. Depending on the fluence, immediate whitening may occur during the treatment which is caused by rapid local heating of the pigment leading to gas or plasma formation and subsequent dermal and epidermal vacuolization. The whitening reaction appears immediately with the use of laser lasting for 20-30 minutes then followed by a scab in 2-5 days. Bleeding indicates excessive fluence and parameters should be adjusted, although pin point bleeding could be acceptable.
Post-procedure, patients must be instructed to apply a petrolatum-based emollient on the treated area until the scab falls off and to allow crusts to slough on their own. The risk of scarring is less than 4.5% with proper use of Q-switched lasers.
Delayed response after laser treatment of Nevus of Ota occurs in some cases, so it is advisable to have a 6-8 weeks interval between the sessions and in case of poor response, to stop the laser treatment and re-evaluate after 3 months.
Picosecond lasers have been suggested to be a more effective tool to treat Nevus of Ota however long term follow up is still lacking.
References
[1] Badawi, A., Osman, M.A. & Kassab, A.N. Behandlung des Naevus Ota und Ito und des Pigmentnävussyndroms. Hautarzt 71, 926-931 (2020). https://doi.org/10.1007/s00105-020-04710-3
[2] Speeckaert, R; Van, Gele, M; Speeckaert, MM; Lambert J; van Geel, N. The biology of hyperpigmentation syndromes. Pigment cell & melanoma research., 2014, 27(4), 512-24.
[3] Lin, JY; Fisher, DE. Melanocyte biology and skin pigmentation. Nature., 2007, 445(7130), 843-50.
[4] Polla, LL; Margolis, RJ; Dover, JS; Whitaker, D; Murphy, GF; Jacques, SL; et al. Melanosomes are a primary target of Q-switched ruby laser irradiation in guinea pig skin. The Journal of investigative dermatology., 1987, 89(3), 281-6.
[5] Anderson, RR; Parrish, JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science (New York, NY)., 1983, 220(4596), 524-7.
[6] Rinaldi, F. Laser: a review. Clinics in dermatology., 2008, 26(6),590-601.
[7] Hruza, GJ; Geronemus, RG; Dover, JS; Arndt, KA. Lasers in dermatology--1993. Archives of dermatology., 1993, 129(8), 1026-35.
[8] Kent, KM; Graber, EM. Laser tattoo removal: a review. Dermatologic surgery:official publication for American Society for Dermatologic Surgery [et al.]., 2012, 38(1),1-13.
[9] Ara, G; Anderson, RR; Mandel, KG; Ottesen, M; Oseroff, AR. Irradiation of pigmented melanoma cells with high intensity pulsed radiation generates acoustic waves and kills cells. Lasers in surgery and medicine., 1990, 10(1),52-9.
[10] Ho, DD; London, R; Zimmerman, GB; Young, DA. Laser-tattoo removal--a study of the mechanism and the optimal treatment strategy via computer simulations. Lasers in surgery and medicine., 2002, 30(5), 389-97.
[11] Herd, RM; Alora, MB; Smoller, B; Arndt, KA; Dover, JS. A clinical and histologic prospective controlled comparative study of the picosecond titanium:sapphire (795 nm) laser versus the Q-switched alexandrite (752 nm) laser for removing tattoo pigment. Journal of the American Academy of Dermatology., 1999, 40(4), 603-6.
[12] Jean, L; Bolognia, JLJ; Julie, V. Schaffer. Dermatology. Third ed., USA: Elsevier, 2012, 2012.
[13] Ho, SG; Chan, NP; Yeung, CK; Shek, SY; Kono, T; Chan, HH. A retrospective analysis of the management of freckles and lentigines using four different pigment lasers on Asian skin. Journal of cosmetic and laser therapy:official publication of the European Society for Laser Dermatology., 2012, 14(2), 74-80.
[14] Kilmer, SL; Wheeland, RG; Goldberg, DJ; Anderson RR. Treatment of epidermal pigmented lesions with the frequency-doubled Q-switched Nd:YAG laser. A controlled, single-impact, dose-response, multicenter trial. Archives of dermatology., 1994, 130(12), 1515-9.
[15] Li, Y; Tong, X; Yang, J; Yang, L; Tao, J; Tu, Y. Q-switched alexandrite laser treatment of facial and labial lentigines associated with Peutz-Jeghers syndrome. Photodermatology, photoimmunology & photomedicine., 2012, 28(4), 196-9.
[16] Trafeli, JP; Kwan, JM; Meehan, KJ; Domankevitz, Y; Gilbert, S; Malomo, K; et al. Use of a long-pulse alexandrite laser in the treatment of superficial pigmented lesions. Dermatologic surgery:official publication for American Society for Dermatologic Surgery [et al.]., 2007, 33(12), 1477-82.
[17] Mariwalla, K; Dover, JS. The use of lasers in the pediatric population. Skin therapy letter., 2005, 10(8), 7-9.
[18] Ho, SG; Yeung, CK; Chan, NP; Shek, SY; Chan, HH. A comparison of Q-switched and long-pulsed alexandrite laser for the treatment of freckles and lentigines in oriental patients. Lasers in surgery and medicine., 2011, 43(2), 108-13.
[19] Choi, CW; Kim, HJ; Lee, HJ; Kim, YH; Kim, WS. Treatment of nevus of Ota using low fluence Q-switched Nd:YAG laser. International journal of dermatology., 2014, 53(7), 861-5.
[20] Kono, T; Nozaki, M; Chan, HH; Mikashima, Y. A retrospective study looking at the long-term complications of Q-switched ruby laser in the treatment of nevus of Ota. Lasers in surgery and medicine., 2001, 29(2), 156-9.
[21] Kono, T; Chan, HH; Ercocen, AR; Kikuchi, Y; Uezono, S; Iwasaka S; et al. Use of Q-switched ruby laser in the treatment of nevus of ota in different age groups. Lasers in surgery and medicine., 2003, 32(5), 391-5.
[22] Chan JC, Shek SY, Kono T, Yeung CK, Chan HH. A retrospective analysis on the management of pigmented lesions using a picosecond 755-nm alexandrite laser in Asians. Lasers Surg Med 2016; 48: 23-29.
[23] Kopera D, Hohenleutner U, Landthaler M. Quality-switched ruby laser treatment of solar lentigines and Becker’s nevus: a histopathological and immunohistochemical study. Dermatology (Basel, Switzerland) 1997; 194: 338-343.
[24] Lowe NJ, Wieder JM, Sawcer D, Burrows P, Chalet M. Nevus of Ota: treatment with high energy fluences of the Q-switched ruby laser. J Am Acad Dermatol 1993; 29: 997-1001
[25] Fusade T, Lafaye S, Laubach HJ. Nevus of Ota in dark skin–an uncommon but treatable entity. Lasers Surg Med 2011; 43: 960-964.
[26] Levin MK, Ng E, Bae YS, Brauer JA, Geronemus RG. Treatment of pigmentary disorders in patients with skin of color with a novel 755 nm picosecond, Q-switched ruby, and Q-switched Nd:YAG nanosecond lasers: a retrospective photographic review. Lasers Surg Med 2016; 48:181-187.
[27] Ohshiro T, Ohshiro T, Sasaki K, Kishi K. Picosecond pulse duration laser treatment for dermal melanocytosis in Asians : a retrospective review. Laser Ther 2016; 25: 99-104.
[28] Chuah SY, Hammami Ghorbel H, Lacour JP, Passeron T. Acquired dermal melanocytosis of the nose. J Eur Acad Dermatol Venereol 2015; 29:827-829.
[29] Mizoguchi M, Murakami F, Ito M et al. Clinical, pathological, and etiologic aspects of acquired dermal melanocytosis. Pigment Cell Res 1997;10: 176-183.
[30] Hori Y, Kawashima M, Oohara K, Kukita A. Acquired, bilateral nevus of Ota-like macules. J Am Acad Dermatol 1984; 10: 961-964.
[31] Park JM, Tsao H, Tsao S. Acquired bilateral nevus of Ota-like macules (Hori nevus): etiologic and therapeutic considerations. J Am Acad Dermatol 2009; 61: 88-93
[32] Bernstein, EF; Kornbluth, S; Brown, DB; Black, J. Treatment of spider veins using a 10 millisecond pulse-duration frequency-doubled neodymium YAG laser. Dermatologic surgery: official publication for American Society for Dermatologic Surgery [et al.]., 1999, 25(4), 316-20.
[33] Kossida, T; Rigopoulos, D; Katsambas, A; Anderson, RR. Optimal tattoo removal in a single laser session based on the method of repeated exposures. Journal of the American Academy of Dermatology., 2012, 66(2), 271-7.
[34] Reddy, KK; Brauer, JA; Anolik, R; Bernstein, L; Brightman, L; Hale E; et al. Topical perfluorodecalin resolves immediate whitening reactions and allows rapid effective multiple pass treatment of tattoos. Lasers in surgery and medicine., 2013, 45(2), 76-80.
[35] Bernstein, EF. Laser treatment of tattoos. Clinics in dermatology., 2006, 24(1), 43-55.
[36] Kilmer, SL; Lee, MS; Grevelink, JM; Flotte, TJ; Anderson, RR. The Q-switched Nd:YAG laser effectively treats tattoos. A controlled, dose-response study. Archives of dermatology., 1993, 129(8), 971-8.
[37] Kilmer, SL. Laser treatment of tattoos. Dermatologic clinics., 1997, 15(3), 409-17.
Помеченный: Лазеры, EBD и Боди шэйп, Клиническая дерматология и дерматологическая хирургия
Rate this article
Share this article on