
Introduction
Minimally invasive breast surgery (breast augmentation) has, in just a few years, become one of the most widely discussed topics in aesthetic breast surgery, extending far beyond the scientific literature alone. Social media platforms (TikTok, Instagram, YouTube) have played a major role in its rise in popularity: as of May 2026, the hashtag #miafemtech had accumulated more than 2.1 million posts, while dozens of patient and surgeon vlogs have promoted the image of a procedure that is quick, painless, and performed with "no visible scar."
The phenomenon has also made its way into plastic surgery conferences, where the MIA FemTech technique (Motiva/Establishment Labs) now occupies an increasingly prominent place. Both The Aesthetic Meeting in Boston and the SOFCEP meeting in Biarritz, held in May 2026, featured lively panel discussions dedicated to the topic, during which surgeons had the opportunity to compare and debate their perspectives.
The impact of this media exposure is evident in clinical practice. Many patients now arrive for consultations specifically requesting this technique after browsing social media, watching online videos, or even consulting generative artificial intelligence before scheduling an appointment.
In these cases, demand precedes medical information—a clear indication that the marketing strategy has been highly effective.
This situation raises a straightforward question: Does minimally invasive breast surgery represent a genuine scientific advancement, or is it simply a marketing success story?
History Repeats Itself
“Those who cannot remember the past are condemned to repeat it.”
The year 2026 has been marked by the return of many familiar trends: the Renault 4L and Renault 5 have been reintroduced as electric vehicles, 1980s jeans are back on fashion runways, and classic songs have been re-released with new orchestrations to great commercial success. In our specialty, it is the prepectoral implant position that is making a major comeback, now presented as an innovation—even though it was the standard approach before 1995.
Before silicone gel breast implants were banned in France, almost all breast implants were placed in the prepectoral plane. It was the introduction of saline-filled implants, along with their well-known drawbacks (rippling, visibility, palpability, and capsular contracture), that led the surgical community to adopt the retropectoral approach during the 2000s. Surgeons who did not practice during that period may understandably perceive this return as a novel advancement.
The Motiva MIA FemTech and Preserve® Techniques
The MIA FemTech technique uses a 2–3 cm transaxillary incision, creates the implant pocket using an inflatable balloon dissector without electrocautery, and introduces the implant through a patented insertion device. The implant is placed in the prepectoral position under local anesthesia, with the entire procedure taking approximately 30 minutes and allowing same-day discharge. The average price currently reported in France is around €9,000.
The truly novel aspects of the technique are limited to the patented insertion device, the balloon-assisted tissue expansion method, and the use of a biconvex breast implant. By contrast, the axillary approach, prepectoral implant placement, and the use of local anesthesia for breast augmentation have all been described in the surgical literature for several decades.
From a scientific standpoint, only one clinical study has been published to date: Chacon-Quiros et al. (Aesthetic Surgery Journal, March 2026), involving 100 patients with 3 years of follow-up and no control group (Level IV evidence). The short-term results are encouraging, with a reported complication rate of 3.2%, but the follow-up is inherently too limited to assess long-term safety. In addition, three of the study's authors disclosed consulting relationships with Establishment Labs.
In response to surgical criticism regarding the lack of direct visualization and the blind creation of the implant pocket, Motiva developed the Preserve® technique, which introduces an inframammary incision together with a modified dissection protocol. The implant pocket is again created using an inflatable balloon dissector but now allows direct visualization during dissection, and the implant is inserted through an insertion sleeve.
Preserve® follows the same commercial model as MIA FemTech, relying on dedicated proprietary instruments, exclusive use of Motiva implants, paid certification training, and mandatory licensing. To date, it has not been supported by any independent clinical studies. Its timing is noteworthy: the technique was introduced precisely as medical criticism of MIA FemTech was becoming more prominent at major plastic surgery meetings. As such, it appears more consistent with a commercial response designed to address these criticisms than with a well-documented surgical innovation.
Drawbacks of Prepectoral Implant Placement
Prepectoral implant placement, which is common to both the MIA FemTech and Preserve® techniques, represents the main area of clinical concern, regardless of any commercial considerations. Its limitations have been well documented in the independent surgical literature for many years, and they are not altered by Motiva's commercial packaging.
The most immediate concern is implant visibility and palpability. Without muscular coverage, the implant lies directly beneath the breast gland and the skin. In patients with a pinch test of less than 2 cm—a profile commonly encountered among candidates for breast augmentation—the implant is more likely to become visible and palpable, compromising the aesthetic result over the medium term.
The risk of capsular contracture is also significantly higher with prepectoral placement than with retropectoral placement. A retrospective study of 392 patients reported rates of 9.9% versus 3.5%, respectively, with comparable follow-up (NCBI, 2024).
Another well-documented limitation is earlier breast ptosis. Without muscular support, the entire weight of the implant is borne by the breast tissue and skin envelope. As a result, sagging tends to occur more rapidly than with retropectoral placement and is further accelerated by pregnancy, breastfeeding, or weight fluctuations—common life events in the age group most likely to undergo breast augmentation.
A more insidious long-term complication is secondary tissue thinning. Chronic pressure exerted by the implant gradually compresses and thins the overlying breast tissue. A result that appears entirely satisfactory at age 30 may evolve into a significant aesthetic failure by age 45 or 50, making revision surgery considerably more complex and carrying greater surgical risk. Rippling, the visible wrinkling of the implant through the skin, is another complication that is closely associated with the prepectoral plane and is uncommon with retropectoral placement. It occurs preferentially in areas with limited soft-tissue coverage and tends to worsen over time.
These complications are not exceptionally rare. Data from the U.S. Food and Drug Administration (FDA) involving 99,993 patients (Coroneos et al., Annals of Surgery, 2019) showed that by 7 years, 35.9% of women with breast implants had experienced a complication or undergone reoperation, and by 10 years, one in five patients had required implant removal or replacement. Breast implant surgery must therefore be evaluated over the long term, which is precisely what even well-conducted three-year studies are unable to assess.
These considerations do not mean that the prepectoral approach has no appropriate indications. There is a specific patient profile for whom it may be a reasonable option: a woman between 30 and 50 years of age, who has completed childbearing, has a pinch test greater than 2 cm, indicating adequate soft-tissue coverage, and seeks only a small implant to improve breast harmony rather than achieve a substantial increase in volume. In this carefully selected setting, the risks associated with prepectoral placement are reduced, and the benefit–risk balance may be favorable.
This is, however, a niche indication for a carefully selected group of patients and should not be regarded as the standard approach for breast augmentation.
Ethical Considerations
Beyond the scientific questions, the MIA technique—and, more broadly, Establishment Labs' commercial model—raises ethical issues that deserve discussion within the plastic surgery community.
The first concerns the commercialization of the surgical procedure itself. To perform the MIA technique, a surgeon must obtain a license from the manufacturer, complete a paid certification program, and commit to participating in a structured commercial ecosystem.
This raises a legitimate question: Is it ethical for a surgical technique—that is, a set of operative maneuvers derived from medical expertise—to be patented, licensed, and monetized by a private company? Surgery is not software. A surgeon's operative technique belongs to medical education, clinical experience, and the scientific community—not to the holder of an industrial patent.
The second issue concerns clinical autonomy and implant selection. The MIA insertion device is designed exclusively for Motiva implants. By adopting this technique, the surgeon effectively relinquishes the freedom to choose the implant best suited to an individual patient's anatomy. Yet this freedom is a fundamental principle of medical practice. Implant selection—including shape, projection, cohesiveness, and volume—should be guided by the patient's needs rather than the constraints of a commercial agreement. A surgeon who is restricted to using implants from a single manufacturer is no longer entirely free in making medical decisions.
The third issue relates to transparency toward patients. When a patient requests the MIA technique after seeing it on TikTok or Instagram, is she informed that the approximately €9,000 fee includes, among other things, the cost of a commercial license, a proprietary insertion device, and manufacturer-mandated implants? Is she aware that a comparable procedure can be performed at a substantially lower cost without any of these commercial constraints?
True informed consent requires that patients receive all relevant information, including the economic implications of the procedure. It also requires disclosure of a reality that marketing messages often omit: any revision surgery, whether performed early because of a procedural complication (such as hematoma, implant malposition, or infection) or years later because of implant aging or changes in the aesthetic result, will require general anesthesia. Local anesthesia therefore applies only to the initial operation. Presenting it as the central advantage of a technique for which the patient is likely to undergo at least one revision during her lifetime is, at best, an omission and, at worst, a deliberately misleading marketing claim.
These observations are not intended to discredit surgeons who perform the MIA procedure in good faith, nor to deny the genuine benefits that the system may provide in terms of training, procedural standardization, or even practice development. Rather, they invite the surgical community to reflect collectively on where the boundary should lie between medical innovation and the commercial capture of surgical practice.
Can the Same Procedure Be Performed Without a Commercial Contract?
The LILA (Low Impact Local Augmentation) technique, developed at Centre 43 Périer in Marseille, shares the same fundamental objectives as MIA: prepectoral breast augmentation under local anesthesia, using a minimal incision and allowing rapid postoperative recovery. It differs, however, in several important technical aspects.
It should be emphasized that the acronym LILA refers solely to a surgical technique that its authors chose to name. It has no commercial affiliation with any manufacturer, requires no licensing agreement, no paid certification program, and no proprietary instruments. LILA is the name of a surgical technique—not a commercial product.
The procedure uses a 2.5–3 cm inframammary incision located within the breast crease, providing direct visualization of the implant pocket. Pocket dissection is performed under continuous direct vision, allowing immediate verification of hemostasis and digital confirmation of the pocket boundaries—advantages that the inherently blind MIA approach cannot structurally provide.
The implant is inserted using a no-touch technique with a standard insertion device (such as the Hydrocone or Keller Funnel). The surgeon retains complete freedom to select the implant best suited to the patient, as any conventional silicone breast implant can be used without dependence on a specific manufacturer.
In this respect, the LILA technique offers the technical advantages attributed to the Preserve® approach while avoiding dedicated proprietary equipment and eliminating the need for commercial licensing.
The following table summarizes the principal differences between the MIA and LILA techniques.
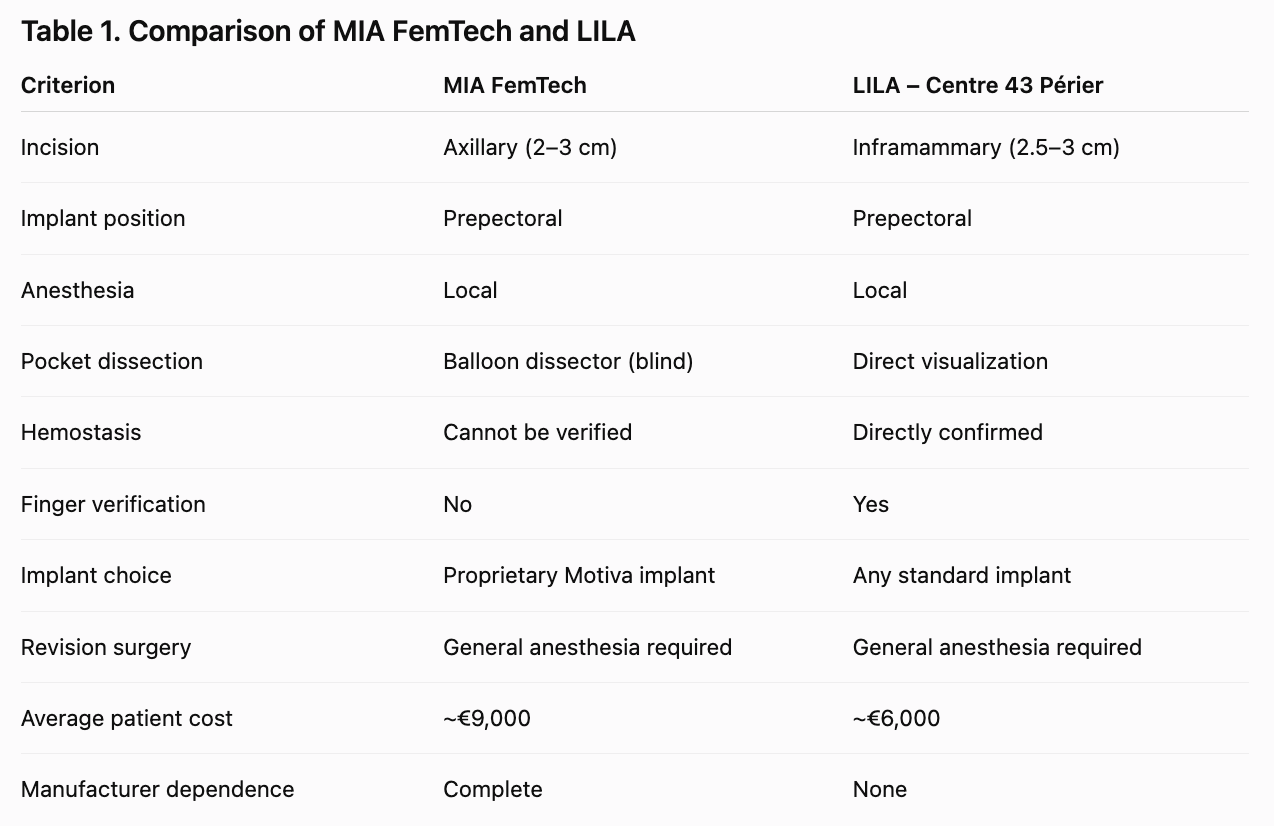
A preliminary series of 10 consecutive cases (November 2025–April 2026) demonstrated high patient satisfaction, no early complications, and aesthetic outcomes comparable to those achieved with MIA. A prospective comparative study is currently underway. The average cost to the patient (approximately €6,000) is substantially lower than that of both the MIA FemTech and Preserve® techniques, a difference directly attributable to the absence of proprietary equipment and licensing fees.
Conclusion
Minimally invasive breast augmentation as promoted through MIA FemTech® and Preserve® is not a surgical revolution. Rather, it represents the return of a well-established prepectoral approach, repackaged through sophisticated industrial design and an undeniably effective digital marketing strategy. The fact that patients increasingly request the procedure by name when attending consultations reflects less a scientific breakthrough than an exceptional marketing success.
Its short-term clinical outcomes appear encouraging; however, the available scientific evidence remains insufficient to establish its long-term safety. The prepectoral approach retains a well-defined niche indication—small-volume breast augmentation in women aged 30 to 50 years, who have completed childbearing and have a pinch test greater than 2 cm—but it should not be promoted as the standard technique for all breast augmentation candidates.
The LILA technique demonstrates that the legitimate goals of minimally invasive breast surgery—patient comfort, local anesthesia, rapid recovery, and a natural aesthetic outcome—can be achieved without reliance on proprietary equipment, without compromising direct surgical control, and at a substantially lower cost.
Ultimately, the surgeon's expertise remains the most important medical device in the operating room.
REFERENCES
1. Chacon-Quiros et al. The 3-Year Results of a 100-Patient Prospective Study of the Safety and Effectiveness of MIA Femtech. Aesthetic Surgery Journal. Vol. 46, No. 3, March 2026.
2. Coroneos CJ, et al. US FDA Breast Implant Postapproval Studies: Long-term Outcomes in 99,993 Patients. Annals of Surgery. 2019;269(1):30–36.
3. U.S. Food and Drug Administration. Executive Summary – General and Plastic Surgery Devices Panel. 2011.
4. NCBI. Prepectoral vs. Retropectoral Breast Augmentation: Comparative Study of 392 Patients. 2024.
被标记: 形体手术, 乳房整形手术, 医疗经营管理
评价这篇文章
分享这篇文章于